There are multiples causes of complex facial deformity including
congenital deformities, cancer resection and trauma. Road accidents,
assaults and sports injuries are common causes of Cranio-Maxillofacial
trauma.
Examples of some of the complex deformities that may be corrected
by modern Cranio-Maxillofacial and reconstructive surgery techniques
are shown below.
| Panfacial
fractures 1
This man crashed his four wheel drive in the Australian
outback and was not found for nearly 24 hours.
He has severe fractures of the lower two thirds of the face. |

|
| |
|
| Panfacial fractures
2
This man crashed his motorbike at high speed. The postoperative
CT shows where I have placed plates at the nasal root, around
the eye sockets, the cheek bones, zygomatic arch and mandible.
The floor of the eye socket has been reformed using hip bone.
The teeth have been wired together to maintain dental occlusion.
|
 |
| |
|
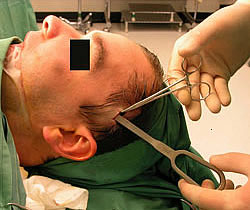
| Submental intubation
This girl sustained multiple facial fractures during an
explosion. I have placed the endotracheal tube beneath the
chin to avoid having a tracheostomy.
I have written a paper about my experiences with submental
intubation in Australian and New Zealand Journal of Surgery. |
 |
| |
|
| Mandible fracture
This boy fractured his lower jaw into 4 pieces in a road
crash.
Both condyles and the parasymphyseal region were plated
into correct alignment.
|
 |
| |
|
Paediatric mandible
fracture
This 5 year old boy fell out of a window fracturing his
lower jaw in 2 places.
Traditional plating would destroy the buds of his adult teeth
and so I repaired the fractures with superficial absorbable
fixation |
 |
| |
|
Condyle fracture
This young girl was assaulted fracturing the condyle of
her mandible.
I have plated this through a submandibular Risdon incision.
|
 |
| |
|
Intracranial condyle
penetration
This man fell over the handlebars of his bicycle and pushed
the condyle of his mandible through the skull base into the
cranial cavity and fractured it on the other side.
I have written a paper about this type of injury in Australian
and New Zealand Journal of Surgery. |
 |
| |
|
TMJ ankylosis
An old injury of the Temporomandibular joint (TMJ) has caused
a fusion or ankylosis.
This is a notoriously difficult condition to treat. |
 |
| |
|
Mandible gunshot
This man was shot in the lower jaw and all bone from the
from angle to angle is missing.
This was reconstructed using a bone free flap from the leg
and a soft tissue free flap from the arm. |
 |
| |
|
Maxillary occlusal
fracture
This man was running from the scene of a crime when he tripped
and sustained this injury.
I aligned his upper teeth and used hip bone to replace the
missing maxillary bone. |
 |
| |
|
Dental Models
Dental models together with occlusal wafers are used for
complicated segmental fractures involving dental segments. |
 |
| |
|
Palatal fracture
This young man was a driver in a high speed boat accident.
Accurate fracture reduction was critical to achieving the
correct bite |
 |
| |
|
Simple zygomatic arch
fracture
This simple arch fracture can be elevated using a Gillies
lift if the periosteum surrounding the fracture is intact. |
 |
| |
|
Gillies lift
An elevator is passed beneath the deep temporal fascia and
under the zygomatic arch then gently elevated.
This is a case I performed in a young man hit with a cricket
ball. |
 |
| |
|
Zygoma fracture
Although this zygoma fracture could be elevated with a Gillies
lift it would not stay in position and I have placed plates
through the mouth to maintain the reduction. |
 |
| |
|
Comminuted zygoma fracture
In this more extensive zygoma fracture, the root of the
zygomatic arch has fractured off in front of the ear. It is
part of a Le Fort III complex fracture. If not corrected,
the face will remain flat and wide.
I plated this using a coronal incision over the top of the
scalp in the hair. Note the fractured nasal septum. |
 |
| |
|
Fractured nose
A fractured nose heals quickly and is best manipulated into
position within the first two weeks after injury. |
 |
| |
|
Old fractured nose
This is a preoperative view of an old fractured nose that
has been incompletely reduced.
The bones must be refractured and the nasal septum straightened.
|
 |
| |
|
Naso-orbito ethmoid
fracture
This young girl has an untreated NOE complex fracture. As
a result she has a depressed “saddle nose” and
telecanthus.
The attachment of the medial canthal tendon must be reattached
to the side of the nose to resuspend the eyelids. |
 |
| |
|
Costochondral graft
nose
This man has a saddle nose deformity following a naso-orbital
ethmoid fracture.
I have harvested a costochondral graft from the ribs and
am about to place this via an intranasal incision. |
 |
| |
|
Retrobulbar haematoma
This elderly lady fell at home bleeding into the soft tissues
behind her eye. Note how much further forward the globe is
on this side.
Surgery is sometimes required to temporarily relieve the
pressure on the globe and subsequent blindness. |
 |
| |
|
Orbital floor blowout
This man was assaulted and the contents of his orbit have
“blown out” into the maxillary sinus.
This must be corrected to prevent double vision and a sunken
eye (enopthalmos). |
 |
| |
|
Orbital floor bone
graft
I am placing a bone graft from the hip to reconstruct the
floor of an eye socket that has been fractured.
Hip bone is easy to contour into the desired shape. |
 |
| |
|
Medial orbital wall
bone graft
This man has a fracture of the medial orbital wall in a
road accident which tethered the medial rectus muscle which
moves the globe.
I have placed a hip bone graft across the fracture site. |
 |
| |
|
Optic nerve transection
This man had a foreign body enter his neck and pass through
his eye socket in a work place accident.
The eye socket has been fractured inwards and the bone has
cut the optic nerve making him blind. |
 |
| |
|
Lateral orbital wall
fracture
I repaired this lateral orbital wall fracture using a combined
temporal and upper blepharoplasty incision |
 |
| |
|
Depressed skull fracture
This young tourist had a depressed skull fracture sustained
during a bomb blast in a terrorist attack on a night club.
He had 25% burns and shrapnel injury.
I have repaired his naso-ethmoid complex fractures and elevated
the skull fractures with a neurosurgeon. Pericranial flaps
were used to repair dural tears. |
 |
| |
|
Frontal sinus fracture
A craniofacial approach has been used to repair this fracture
of the frontal sinus.
The posterior wall was removed and all the frontal sinus
space turned into part of the cranial cavity. |
 |
| |
|
Tension pneumocephalus
This is a possible complication of frontal sinus fractures.
Air in the nose under high pressure is forced into the cranial
cavity but cannot escape and the brain becomes increasingly
compressed |
 |
| |
|
Mucocoele
Another complication of untreated frontal sinus fracture
when the sinus cannot drain properly.
Mucous produced in the sinus forces its way out into the
forehead soft tissue but can also go into the orbit or the
cranial cavity. |
 |
| |
|
Lacrimal mucocoele
This mucocoele formed when the tear drainage of the lacrimal
sac was interrupted by a maxillary fracture.
An alternative tear drainage into the nasal cavity was created. |
 |
| |
|
Decompressive craniotomy
This young girl in a road accident had severe intracranial
swelling caused by blunt cranial trauma.
The front part of her skull was removed to prevent high pressure
on the brain tissue causing death. Her skull was kept in a
freezer and then replaced three months later. |
 |
